
Most dental practices manage denials reactively. A claim comes back rejected. Someone looks at the reason code, makes a correction, and resubmits. This process feels like billing management. It isn’t.
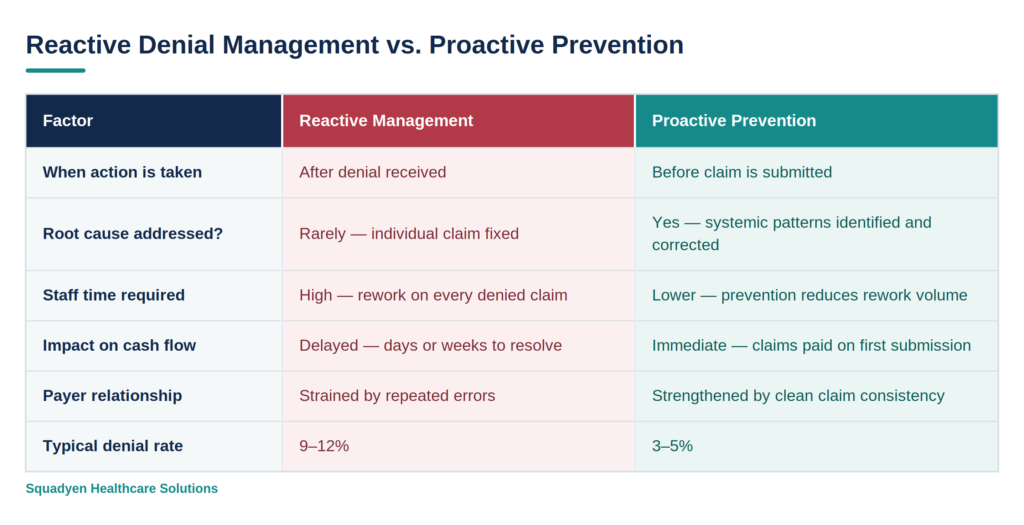
Reactive denial management is damage control. The claim was already denied. The payer relationship has already registered the error. The cash flow has already taken the hit. And in most cases, the same error will happen again next week — because the root cause was never addressed.
This article covers the seven causes of dental claim denials that most billing teams treat as routine problems rather than systemic signals. Understanding them is the difference between a 10% denial rate and a 4% denial rate.
Why Dental Claim Denials Deserve More Attention Than They Get
The industry average claim denial rate for dental practices is 9–10%. Best-performing practices run denial rates of 3–5%. That 5–7 percentage point gap translates to a very large dollar figure at most practice scales.
For a dental practice billing $200,000 per month, the difference between a 9% and a 4% denial rate is $10,000 per month in claims that either require expensive rework or get written off entirely. Over a year, that is $120,000 — roughly the annual cost of a full-time associate.
The 7 Denial Causes Most Billing Teams Miss
Cause 1: Eligibility Verified as ‘Active’ — Benefits Not Confirmed
This is the single most common and most preventable cause of dental claim denials. Confirming that a patient’s insurance is active tells you almost nothing about whether a specific procedure will be reimbursed. The specific details that determine reimbursability — annual maximum remaining, frequency limitations, waiting periods, missing tooth clauses, deductible status — require a full benefits verification, not a coverage check.
When a patient arrives having been told their insurance covers 80% of a crown, but the plan’s annual maximum was already exhausted in January, the claim will either be denied or reduced to $0 patient benefit. This isn’t a payer problem. It’s a verification problem — and it was entirely preventable.
Cause 2: CDT Code Not Supported by Clinical Documentation
Insurance payers are increasingly reviewing clinical notes before reimbursing higher-value procedures — particularly periodontal, endodontic, and restorative claims. When the documentation doesn’t explicitly support the specificity of the code billed, the payer either downcodes the claim or denies it outright.
Common examples: billing D4341 (scaling and root planing) without documented probing depths that clinically justify the procedure; billing D2710 (resin-based composite crown) without clinical notes documenting the necessity and extent of coverage; submitting D0330 (panoramic radiograph) without a documented clinical indication.
Cause 3: NPI Error — Group vs. Individual
Healthcare providers have two National Provider Identifiers: an individual NPI (Type 1) and, if they practice within a group, a group NPI (Type 2). Many payers require the individual NPI in the rendering provider field and the group NPI in the billing provider field. When these are transposed — group NPI in the rendering field, or individual NPI where group is required — the claim is rejected as a billing error.
This error is particularly common when a new provider joins a practice and their individual NPI hasn’t been correctly configured in the practice management system. Every claim they submit until the error is corrected will be rejected.
Cause 4: Missing or Expired Prior Authorisation
For procedures that require prior authorisation — orthodontics, implants, oral surgery, certain restorative services — submitting a claim without a valid authorisation number is an automatic denial. The most common failure modes are: the authorisation was never requested, the authorisation was approved but the number wasn’t recorded in the patient chart, or the authorisation expired before the procedure was completed.
Prior authorisation tracking is a process discipline, not a billing function. The practice management system must flag procedures that require auth, record the approval number and expiry date, and alert the scheduling team if an appointment is scheduled outside the authorisation window.
Cause 5: Timely Filing Limit Exceeded
Every insurance payer sets a timely filing limit — the deadline by which a claim must be submitted after the date of service. These range from 90 days (some Medicare Advantage plans) to 12 months (most commercial payers) to 24 months (original Medicare). Claims submitted after the timely filing limit are denied and generally cannot be appealed on clinical grounds.
Timely filing denials almost always indicate a tracking failure — specifically, a claim that was submitted, rejected for an administrative reason, and then sat in the denial queue without being reworked until the filing window closed. This is why denial management cadence matters: every denied claim needs a next action and a next action date assigned within 48 hours.
Cause 6: Coordination of Benefits Errors on Dual-Coverage Patients
When a patient carries dental coverage under two insurance plans, the claims must be submitted in the correct order — primary first, then secondary after the primary EOB is received. The secondary claim must include the primary EOB as an attachment. The coordination of benefits (COB) rules, which determine which plan is primary, must be applied correctly.
COB errors cause denials at multiple stages: the primary claim is submitted to the wrong payer, the secondary claim is submitted before the primary EOB arrives, the primary EOB is attached to the secondary claim incorrectly, or the COB order in the practice management system doesn’t match what either payer has on file.
Cause 7: Fee Schedule Mismatch Triggering Zero-Benefit Calculation
When a practice bills at a rate higher than the contracted fee schedule, some payers apply the contractual adjustment first and then apply the patient’s benefit percentage to the contracted rate — leaving the patient with a higher-than-expected balance. In certain plan structures, billing above the contracted rate can trigger a zero-benefit calculation, effectively turning a reimbursable claim into a non-covered service.
This denial type is particularly insidious because it doesn’t always show up as an outright denial. The claim may appear ‘paid’ with a $0 insurance benefit, requiring the full balance to be collected from the patient — who then disputes the bill because they expected partial insurance coverage.
Every denial arrives with a reason code. Most billing teams note the code, make the correction, and move on. The practices that achieve sub-5% denial rates do something different — they aggregate reason codes monthly, look for patterns, and trace those patterns back to their root cause in the workflow.
Co-Founder - Squadyen Healthcare Solutions
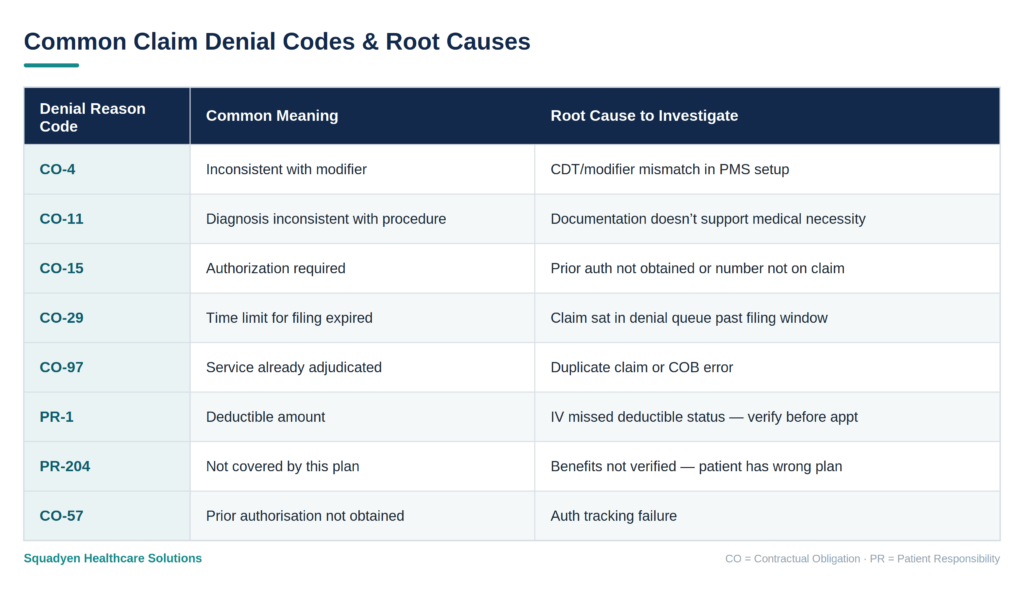
Denial Reason Codes: Your Diagnostic Tool
Building a Denial Prevention System
Denial management reacts to what went wrong. Denial prevention removes the conditions that allow it to go wrong in the first place. Here is the operational structure that best-performing dental practices use:
- Full benefits verification — not just active coverage — completed the day before every appointment
- Clinical documentation review protocol — provider reviews notes against CDT code before claim submission
- Prior authorisation tracker — integrated into the scheduling system, not managed separately
- 48-hour denial rework rule — every denial gets a next action assigned within two business days
- Monthly denial pattern review — aggregate denial reason codes by payer and by provider to identify systemic issues
- Fee schedule audit — contracted rates reviewed annually and updated in the practice management system
This is not a software problem. It is a process discipline problem — and it requires someone accountable for each step.
Reactive vs. Proactive Denial Management: A Comparison
Frequently Asked Questions
Q: What is the average dental claim denial rate and what should mine be?
The industry average is 9–10%. Best-performing dental practices maintain denial rates of 3–5%. If your rate is above 8%, you have systemic process problems — not just individual claim errors — worth investigating. Denial rates above 12% typically indicate multiple concurrent front-end failures.
Q: Can denied dental claims always be appealed?
Not always. Claims denied for timely filing after the deadline generally cannot be successfully appealed on clinical grounds. Claims denied for missing documentation, coding errors, or authorisation issues can almost always be resubmitted with corrections. The key is acting within the payer’s appeal window — typically 90 to 180 days from the denial date.
Q: How do I know which denial cause is most affecting my practice?
Pull your denial report and sort by reason code frequency. Your top three denial codes represent your highest-impact systemic problems. For each code, trace back to the point in the workflow where that error originates — and fix the process at that point, not the individual claim.
Squadyen helps dental practices identify their top denial patterns, implement prevention workflows, and build the reporting discipline needed to keep denial rates consistently below 5%. Talk to our team today!